Segmental Instability
Understanding the Symptoms, Causes & Treatment Options for Spinal Instability
Reviewed by: Dr. Christopher Good, Dr. Colin Haines, Dr. Ehsan Jazini
Your spine is designed to move, but that movement needs to be controlled. When one level of the spine moves more than it should, it can place extra stress on the discs, joints, muscles, and nerves around it. This is known as segmental instability.
For some people, segmental instability feels like recurring low back pain that flares with bending, lifting, or certain movements. For others, it can cause leg pain, numbness, tingling, weakness, or the feeling that the back is “giving out.” Because these symptoms can overlap with other spine conditions, an accurate diagnosis is the first step toward lasting relief.
At VSI, our spine specialists evaluate segmental instability with a personalized approach that looks at your symptoms, movement patterns, imaging, nerve function, and overall spine health — so treatment can be matched to the true source of your pain.
Segmental Instability: Quick Facts
- Segmental instability is abnormal or excessive motion between two vertebrae in the spine.
- It most often affects the lumbar spine, or lower back, but it can also occur in the cervical or thoracic spine.
- It may develop when a disc, facet joint, ligament, muscle, or prior spinal condition can no longer support normal motion.
- Common symptoms include recurring low back pain, stiffness, muscle spasms, radiating leg pain, numbness, tingling, weakness, or a feeling that the back is “giving out.”
- Segmental instability can be caused by disc degeneration, arthritis, spondylolysis, spondylolisthesis, trauma, prior spine surgery, weak core muscles, or congenital spine differences.
- Diagnosis usually involves a medical history, physical exam, movement-based testing, X-rays, flexion-extension imaging, and sometimes MRI or CT scans.
- Treatment usually starts with non-surgical care, including spine-specialized physical therapy, core stabilization, anti-inflammatory medication, activity modification, low-impact exercise, manual therapy, and dry needling when appropriate.
- Surgery may be considered when instability is severe, pain is disabling, nerve symptoms are progressing, or non-surgical treatment has not provided enough relief.
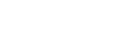
What is Segmental Instability?
To understand segmental instability, it helps to understand how the spine is built.
The spine is made up of bones, discs, soft tissues, joints, and nerves. There are 7 cervical vertebrae in the neck, 12 thoracic vertebrae in the mid-back, and 5 lumbar vertebrae in the lower back. These bones stack on top of one another to support the body while still allowing the spine to bend, twist, and move.
Each level of the spine functions as a three-joint complex. This includes:
- One intervertebral disc in the front
- Two facet joints in the back
Together, the disc and facet joints act like a tripod. They support the weight above that spinal level while allowing controlled movement. When one part of this system weakens, degenerates, loosens, or becomes injured, that spinal level may start to move more than it should.
That excessive motion is called segmental instability.
Segmental instability often develops when a disc or facet joint has degenerated to the point that it can no longer support normal spinal loading. It may also occur with spondylolysis, spondylolisthesis, trauma, weak spinal stabilizing muscles, or changes after prior spine surgery.
The result is not simply “too much flexibility.” It is motion that the spine can no longer control well and that can lead to pain, muscle guarding, nerve irritation, and changes in posture or movement.
Segmental Instability vs Spinal Hypermobility
People often use terms like spinal instability, spine hypermobility, and hypermobility back pain interchangeably. They are related, but they are not always the same.
Some people naturally have more motion in their joints and never develop pain. Others may have extra motion at one spinal level that becomes painful because the surrounding discs, joints, ligaments, muscles, or nerves can no longer control that movement.
|
Term |
What It Means |
Why It Matters |
|
Spinal Hypermobility |
A spinal segment moves more than average |
It is not always painful or dangerous |
|
Functional Instability |
The spine has trouble controlling motion, even if imaging does not show obvious slippage |
Often treated with stabilization-focused physical therapy |
|
Structural Instability |
A disc, facet joint, ligament, fracture, or spinal segment shows measurable abnormal motion or damage |
May require imaging-based monitoring or surgical evaluation |
|
Segmental Instability |
Excessive motion at one spinal level that causes pain, nerve irritation, deformity, or functional limitation |
May require imaging-based monitoring or surgical evaluation |
The key question is not just whether your spine moves more than average. The more important question is whether that motion is causing pain, nerve symptoms, loss of function, or progressive changes in the spine.

Common Symptoms of Spine Instability
Symptoms of segmental instability vary depending on the location and severity of the unstable spinal segment. In many patients, symptoms are mechanical, meaning they change with movement, posture, or activity.
Common symptoms may include:
- Recurring low back pain
- Pain that worsens with bending, lifting, twisting, or changing positions
- Stiffness in the lower back
- Muscle spasms or tightness
- A catching, locking, shifting, or “giving out” sensation in the back
- Pain when getting up from a chair
- Pain when rolling over in bed
- Pain that improves temporarily when lying down or changing position
- Pain that radiates into the buttocks, hips, or legs
- Numbness, tingling, pain, or weakness in the legs
- Difficulty standing or walking for long periods
- Trouble trusting your back during normal daily activities
When instability places pressure on spinal nerves, patients may also develop symptoms of radiculopathy, including pain, numbness, tingling, or weakness that travels into the leg.
When Symptoms May Be an Emergency
Severe spinal instability or nerve compression can rarely lead to cauda equina syndrome, which is a medical emergency.
Seek immediate medical evaluation if you experience:
- Loss of bowel or bladder control
- New urinary urgency or inability to urinate
- Numbness around the groin or saddle area
- New or worsening weakness in the legs
- Difficulty with balance or walking
Unclear on Hypermobility Spine Symptoms?
Schedule a consultation with VSI for a detailed evaluation and accurate diagnosis by speaking with our spine doctors. We recommend in-person visits for the best care.
When Should You See a Spine Specialist?
Occasional back soreness can happen after exercise, travel, lifting, or a long day on your feet. But pain that persists, keeps returning, or comes with nerve symptoms deserves a closer look.
You should consider scheduling an evaluation if:
- Back pain lasts longer than 10 days
- Pain keeps coming back with normal activity
- You feel like your back is unstable or giving out
- Pain is interfering with work, exercise, sleep, or daily life
- You have numbness, tingling, pain, or weakness in the legs
- Symptoms worsen with bending, lifting, or changing positions
- You have a history of spondylolysis, spondylolisthesis, disc degeneration, trauma, or prior spine surgery
- You have been told you may need surgery but want a complete evaluation of all options
Early evaluation can help identify the source of the problem before symptoms become more limiting. It can also help patients access a wider range of non-surgical and surgical treatment options.

What Causes Segmental Instability?
Segmental instability can develop for several reasons. In many cases, more than one factor is involved.
Degenerative Causes
Degeneration is one of the most common reasons a spinal segment becomes unstable. Over time, the disc and facet joints can lose their normal structure and strength. When this happens, the spine may have a harder time maintaining controlled motion.
Degenerative causes may include:
- Degenerative disc disease
- Loss of disc height
- Facet joint arthritis
- Ligament laxity
- Degenerative spondylolisthesis
- Disc collapse or abnormal loading across one level of the spine
Structural or Developmental Causes
Some patients are born with spinal anatomy that increases stress across certain areas of the spine. Others develop structural issues over time.
Structural causes may include:
- Spondylolysis
- Spondylolisthesis
- Scoliosis or spinal alignment changes
- Congenital spine differences
- Generalized joint laxity or connective tissue conditions
Muscle and Movement-Control Causes
The spine relies on strong, coordinated muscles to stay stable during movement. When the deep core and back stabilizers are weak, delayed, or poorly coordinated, the spine may compensate with painful movement patterns.
Contributors may include:
- Weak core muscles
- Poor multifidus activation
- Weak glutes or hip stabilizers
- Deconditioning
- Poor posture or body mechanics
- Repetitive bending, lifting, or twisting
- Reduced control during sports or work activities
Injury-Related Causes
Trauma can damage the bones, joints, discs, or ligaments that help stabilize the spine. Injury-related causes may include:
- Falls
- Car accidents
- Sports injuries
- Repetitive microtrauma
- High-impact loading
- Severe cervical or thoracic trauma
Postsurgical Causes
In some cases, instability may develop after prior spine surgery, especially when a spinal level has changed the way nearby segments move or bear load.
Postsurgical causes may include:
- Prior decompression
- Prior laminectomy
- Prior discectomy
- Adjacent segment stress after fusion
- Changes in spinal alignment after surgery
Understanding the cause matters because treatment should be tailored to the reason the spine is unstable. A patient with muscle-control instability may need a different plan than someone with progressive spondylolisthesis, nerve compression, or instability after prior surgery.
How Is Segmental Instability Diagnosed?
Segmental instability should not be diagnosed from symptoms alone. Back pain, leg pain, stiffness, and spasms can come from many different conditions, including disc herniation, spinal stenosis, degenerative disc disease, arthritis, sacroiliac joint dysfunction, and muscle injury.
At VSI, diagnosis begins with a detailed history and comprehensive physical examination, then uses imaging to evaluate how the spine behaves under load and in motion.
Medical History
Your specialist will ask about:
- Where your pain is located
- When symptoms started
- What movements make pain better or worse
- Whether you feel catching, shifting, locking, or giving way
- Whether pain travels into the leg
- Whether you have numbness, tingling, or weakness
- Prior injuries, surgeries, or spine diagnoses
- How symptoms affect work, sleep, exercise, and daily life
These details help your doctor understand whether symptoms behave like mechanical instability, nerve compression, inflammation, or another spine condition.
Physical Exam
A physical exam helps evaluate movement, strength, nerve function, posture, and pain patterns. Your exam may include:
- Range-of-motion testing
- Strength testing
- Reflex testing
- Sensation testing
- Gait and balance assessment
- Pain provocation testing
- Sit-to-stand movement assessment
- Evaluation of spinal alignment and posture
- Segmental motion testing
- Assessment of core and hip stability
Certain findings may raise suspicion for instability, such as painful movement transitions, a catching sensation, difficulty returning upright from bending, or pain that changes when muscles are activated.
No single exam test confirms segmental instability by itself. Diagnosis is based on the full pattern of symptoms, exam findings, and imaging.
X-Rays and Flexion-Extension Imaging
Imaging is essential when segmental instability is suspected. Typical X-rays may include:
- Weight-bearing AP views
- Lateral views
- Flexion views
- Extension views
Flexion-extension X-rays are especially important because they show the spine in motion. A standard X-ray may look relatively normal, but bending forward and backward can reveal abnormal movement between vertebrae.
This helps determine whether one spinal segment is shifting, slipping, or moving more than it should.
MRI or CT Scans
MRI and CT scans may also be used depending on the patient’s symptoms and history. An MRI can help evaluate:
- Discs
- Nerves
- Spinal canal narrowing
- Disc herniation
- Inflammation
- Soft tissue changes
- Signs of nerve compression
A CT scan can be helpful for:
- Bone detail
- Fractures
- Prior fusion or surgical hardware
- Complex anatomy
- Trauma evaluation
Imaging findings are always interpreted alongside your symptoms and physical exam. Not every imaging abnormality causes pain, and not every painful instability pattern is obvious in one image.
Conditions That Can Feel Like Segmental Instability
Segmental instability can mimic other spine, hip, and nerve-related conditions. This is one reason a careful diagnosis is so important.
|
Condition |
How It Can Feel Similar |
How It May Be Different |
|
Back pain with leg pain, numbness, tingling, or weakness |
Often more nerve-pattern dominant |
|
|
Back and leg symptoms, walking difficulty, weakness |
Often worse with standing or walking and better with sitting or bending forward |
|
|
Vertebral slippage, back pain, leg symptoms |
May be a cause or result of instability |
|
|
Mechanical low back pain, stiffness, disc collapse |
May contribute to instability but can exist without abnormal motion |
|
|
Back pain, stiffness, pain with extension |
Often joint-driven rather than motion-instability driven |
|
|
Low back, buttock, hip, or groin pain |
Pain source is the SI joint rather than a spinal motion segment |
|
|
Muscle Strain |
Back pain and spasm |
Usually improves with time and does not involve abnormal vertebral motion |
At VSI, we look beyond the label and focus on identifying the true pain generator. Many patients have more than one contributing issue, which is why a personalized diagnostic process matters.
What Are Common Treatments for Segmental Instability?
Treatment for segmental instability depends on the severity of the instability, the cause of the abnormal motion, whether nerves are involved, and how much symptoms are affecting daily life.
Most patients begin with non-surgical treatment.
Non-Surgical Treatment
Initial treatment may include:
- Spine-specialized physical therapy
- Anti-inflammatory medication when appropriate
- Core strengthening
- Low-impact exercise
- Manual therapy
- Massage therapy
- Dry needling
- Activity modification
- Posture and body mechanics training
- Injections when pain or inflammation limits progress
The goal is not simply to rest the spine. The goal is to help the spine move with better control.
Surgical Treatment
When a patient’s pain gets too severe or isn’t resolved with non-surgical solutions, it becomes time to meet with a surgeon who can help decide if surgery, such a stabilizing fusion, is appropriate to provide relief.

For many patients, the most important part of treatment is rebuilding the support system around the unstable segment. This often includes strengthening the deep core muscles, multifidus, glutes, hips, and other stabilizers that help protect the spine during everyday movement.
Treatment Pathway
|
Treatment Stage |
Best For |
What It May Include |
Goal |
|
Activity Modification |
Pain flares or early symptoms |
Avoiding painful loading, reducing twisting, changing sitting/lifting mechanics |
Calm symptoms while staying safely active |
|
Pain flares or early symptoms |
Core stabilization, multifidus training, hip/glute strengthening, movement retraining |
Improve control of the unstable segment |
|
|
Medication |
Short-term pain or inflammation |
Anti-inflammatory medication or other medications when appropriate |
Reduce pain enough to participate in physical therapy |
|
Pain that limits physical therapy or overlaps with nerve/facet inflammation |
Targeted injections depending on the pain source |
Reduce inflammation and clarify the pain generator |
|
|
Muscle guarding or movement restriction |
Hands-on therapy, massage, dry needling when appropriate |
Improve mobility and reduce protective muscle tension |
|
|
Severe instability, progressive nerve symptoms, deformity, or failed conservative care |
Spinal fusion surgery or other stabilization options depending on anatomy |
Stabilize the painful segment and protect nerves |
Not every patient needs every step. Some patients improve with physical therapy and activity changes. Others may need injections, advanced imaging, or surgical evaluation if symptoms persist or worsen.
What Activities Should You Avoid With Segmental Instability?
Activity recommendations should be personalized, but certain movements may aggravate spinal instability, especially during a flare-up.
You may need to avoid or modify:
- Heavy lifting with poor form
- Repetitive bending and twisting
- Loaded forward flexion
- High-impact sports during painful flare-ups
- Diving, gymnastics, or contact sports unless cleared by a clinician
- Sudden twisting or extension movements
- Prolonged sitting without support
- Pushing through sharp or radiating pain
- Returning to sports or heavy training before stability improves
The goal is not to stop moving altogether. In most cases, staying active in a controlled way is better than prolonged rest. A spine-specialized physical therapist can help you understand which movements are safe, which should be modified, and how to return to activity with better spinal control.
What Exercises Help Stabilize the Spine?
The right exercises depend on the cause and severity of instability. In general, treatment often focuses on improving control, strength, and endurance in the muscles that support the spine.
A physical therapy plan may include:
- Deep core activation
- Multifidus strengthening
- Transverse abdominis training
- Glute strengthening
- Hip mobility work
- Neutral-spine control
- Balance and proprioception training
- Low-impact conditioning
- Walking, cycling, or aquatic therapy when tolerated
- Functional movement training for bending, lifting, and daily activity
Your core is more than your abdominal muscles. It includes the diaphragm at the top, pelvic floor at the bottom, abdominal muscles in the front, and deep spinal muscles in the back. These muscles work together to support the spine during movement.
At VSI, physical therapy is designed to help patients build strength that carries over into real life — not just exercises that feel good in the clinic.
When Is Surgery Considered for Segmental Instability?
A diagnosis of segmental instability does not automatically mean surgery is required.
Surgery is usually considered when:
- Non-surgical treatment has not provided meaningful relief
- Instability is confirmed on imaging and matches the patient’s symptoms
- Pain is severe and functionally limiting
- Nerve compression is causing progressive weakness, numbness, or walking problems
- A vertebra is slipping or moving abnormally
- Spinal alignment is worsening
- Symptoms are interfering with daily life despite appropriate conservative care
When surgery is recommended, the goal is to stabilize the painful motion segment, reduce abnormal movement, protect the nerves, and improve alignment.
Spinal Fusion for Segmental Instability
For severe instability, spinal fusion may be recommended. Spinal fusion surgery joins two vertebrae together so they heal into one stable segment. This prevents further painful motion or slippage at that level.
A fusion may also help restore alignment and disc height when instability has caused structural changes in the spine.
Some patients need decompression to relieve pressure on nerves. Others need stabilization. Some may need both, depending on the cause of symptoms and the anatomy involved.
The right surgical plan should be customized to the patient, not based on imaging alone.
Can Segmental Instability Improve Without Surgery?
Yes, some cases of segmental instability can improve without surgery, especially when symptoms are caught early and the unstable segment can be supported through targeted rehabilitation.
Non-surgical care may help by:
- Reducing inflammation
- Improving core and hip stability
- Reducing painful movement patterns
- Improving posture and lifting mechanics
- Building endurance in spinal stabilizing muscles
- Helping the patient return to activity safely
However, recovery depends on the cause and severity of instability. Structural instability from significant disc collapse, spondylolisthesis, trauma, deformity, or prior surgery may require closer monitoring and, in some cases, surgical stabilization.
Outlook and Recovery
Recovery from segmental instability looks different for every patient.
Mild or early instability may improve with physical therapy, activity changes, and a structured strengthening plan. More advanced instability may require injections, bracing, pain management, or surgical evaluation.
In general:
- Early symptoms may respond well to conservative care.
- Recurring pain may improve when the spine’s stabilizing muscles are retrained.
- Symptoms can return if the spine is repeatedly overloaded before strength and control improve.
- Nerve symptoms should be evaluated carefully, especially if weakness is present.
- Surgery is usually reserved for confirmed instability with disabling pain, worsening nerve symptoms, or failure of non-surgical treatment.
The most important step is understanding why your spine is unstable and what treatment option best fits your condition.
How VSI Treats Segmental Instability
Segmental instability is not a one-size-fits-all diagnosis. Two patients can have similar imaging findings but very different symptoms, activity goals, and treatment needs.
At VSI, our team evaluates the full spine, not just one image or one painful area. We consider how the discs, facet joints, nerves, muscles, posture, prior injuries, and movement patterns all work together.
Our approach may include:
- Advanced diagnostic imaging
- Flexion-extension X-rays
- Spine-specialized physical therapy
- Non-surgical pain management
- Regenerative medicine options when appropriate
- Injections when indicated
- Surgical expertise when instability is severe or persistent
- A personalized recovery plan through Recovery Revolution™
Whether your path involves physical therapy, injections, surgery, or a combination of treatments, the goal is the same: to help you move with more confidence, less pain, and a clearer understanding of what your spine needs.
Your Path to Relief Starts Here
You may be dealing with ongoing pain, uncertainty, or a recent diagnosis. Our team specializes in diagnosing and treating segmental instability with both non-surgical and surgical options.
The best next step is a personalized evaluation. VSI offers same-week appointment availability and no referrals are needed.
Meet the Specialists Who Treat Segmental Instability
Our team includes board-certified spine specialists with extensive experience diagnosing and treating segmental instability. Each physician takes a personalized approach, combining advanced imaging, non-surgical therapies, physical therapy, and when necessary, surgical expertise to deliver the best possible outcome.

Dr. Niteesh Bharara is a double-board certified physiatrist who is recognized in the top 7% of physicians in the United States. Leading the Mid-Atlantic region in regenerative therapies and injections such as stem cell therapy, PRP therapy, VIA Disc and adipose fat injections, he’s earned the title of Face of Regenerative Medicine by Washingtonian Magazine and Top Doctor recognition in consecutive years.





